Inpatient Services – Tina O’Brien
Transcript
Hi, my name is Tina O’Brien. I’m the Peer support coordinator for the City of Lake Mary fire department. One of the most stressful situations that you and your team may encounter is a member in crisis. It is critical to ensure they find the best treatment while maintaining their dignity, confidentiality, and offering a sense of hope to someone who may have very little. In this module, we will discuss in-patient treatment centers, what to look for in these facilities, how to address concerns you may have, and how a first responder in-patient treatment program may look. Having a predetermined plan and protocol in place will help reduce the stress in what may be the most stressful day your member has experienced and set them up for the greatest chance of success and well-being.
Inpatient – Course Chapters
1. Behavioral Health Overview
Audio
Transcript
Inpatient Behavioral Health Services
Inpatient Behavioral Health Services. This module of the Toolkit serves to provide information necessary for establishing or improving your organization’s Behavioral Health Access Program, with a focus on Inpatient Services.
The objectives for this module are to: learn about behavioral health and why it matters, gain information about growing the inpatient component of your behavioral health access program, learn about special considerations and vetting inpatient providers, and explore common barriers to care and issues related to continuity of care.

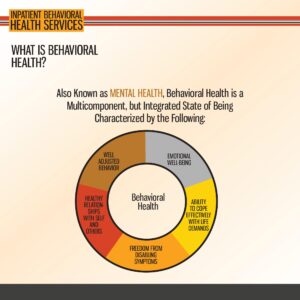
What is Behavioral Health?
If you have already completed the Outpatient Services module of the Toolkit, you may notice some overlap of information in this module. Though this may seem like an oversight, we assure you that it is very much intentional. The reason for this overlap is that both outpatient and inpatient services components of your Behavioral Health Access Program are likely to be stronger and more effective if they are both built on the same foundational understanding of what behavioral health is and is not. By reinforcing this understanding throughout all levels of the Behavioral Health Access Program, we have the opportunity to reduce stigma associated with help seeking and normalize behavioral health as human health! So, before we move on, let us briefly review what is meant by the concept of behavioral health. As this image shows, behavioral health, which is commonly referred to as mental health, is comprised of multiple components that come together to make each of us who we are. It includes our external behavior, our emotions, our relationships with self and others, and our ability to deal effectively with responsibilities and stress. It also includes any symptoms that we may experience physically and/or psychologically. Each component can influence the others. Though this can feel like a negative thing, such as when we get a bad night of sleep and it seems to make everything worse the following day, it more often than not is a good thing. Positive changes we make in one area typically make us more resilient in others. We encourage you to take a moment to reflect on this conceptualization of behavioral health and how it relates to your life. Are there areas where you’re really satisfied? Are there areas that could use some improvements? Regardless of your answers, we can guarantee you, you’re not alone. People are constantly fluctuating to some degree in all areas. It just means we’re all human.
What is Behavioral Health?
Now that we’ve reviewed what behavioral health is, let us also briefly review what it is not. We won’t belabor the point too long as your participation in this training proves that you are approaching the topic of behavioral health with an open mind. However, this isn’t the case for everyone. Though behavioral health is as old as mankind itself, our collective understanding and treatment of it has not always been the best. For too long, behavioral health has been stigmatized, feared, or ignored. This is particularly true among first responders and other cultures who pride themselves on mental and physical strength, courage, and self‑reliance. These are admirable qualities, but sadly an over emphasis on these qualities has left many feeling broken, weak, incompetent, ashamed or stupid for experiencing natural, human emotions due to the extremely challenging experiences they have serving on the frontlines of the modern‑day world. We are here today to change that narrative. We are here to let first responders know that it is completely understandable that they would be impacted by the immense demands placed upon them by the nature of their professions, but that there is hope. Hope for a better future, even for those experiencing the most severe or disabling symptoms. It may feel dark, heavy, or lonely, but none of these things has to become a permanent state of existence. There are others out there who have also felt the weight of those same demands before, but they are still here, living testaments, that with the right support, first responders can heal and get back to enjoying fulfilling, purpose guided lives. As we continue with this module, we will repeatedly emphasize this message as it is of particular significance when we are helping team members who may require Inpatient Behavioral Health Services.
2. BHAP Framework
Audio
Transcript
Growing Your Program
If asked about their perceptions of inpatient behavioral health services, many people may describe bleak images from movies or other media in which patients are retained in prison‑like environments, dressed in stained covered hospital gowns, and medicated to the point of near catatonia. These images have contributed to inpatient mental health services becoming highly stigmatized and considered as an option reserved only for those experiencing acute states of psychosis. However, the goal of this presentation is to correct misconceptions about inpatient mental health services and to provide you a better understanding of why inpatient behavioral health resources are a critical component to any comprehensive Behavioral Health Access Program.
We hope to achieve this goal by first reviewing the levels of care as set forth by the Behavioral Health Access Program framework and reasons why each of these levels matter. Afterwards we will review the steps for growing your organization’s Behavioral Health Access Program and the special considerations that should be made when doing so. As this module pertains to inpatient services, particular focus will be paid to those considerations relevant to this level of care. You will be provided helpful information regarding the qualities to look for in an inpatient service provider as well as suggested questions to ask when conducting your own vetting process. In conclusion, we will discuss the best practices for supporting a member who has been recently discharged from inpatient behavioral health services and why this follow through is so incredibly important to not only the wellbeing of the member, but the organization as a whole.
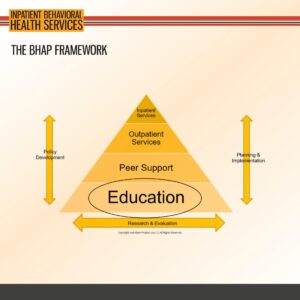
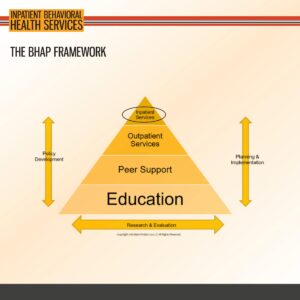
In this illustration, provided courtesy of 2nd Alarm Project, a comprehensive Behavioral Health Access Program is conceptualized as a pyramid. Each layer of the pyramid facilitates and supports the adjacent layers. Additionally, all layers are flanked on each side by the crucial elements of policy development, planning and implementation, and research and evaluation. Though we won’t go into each layer of this framework in detail, it is still helpful to understand the broader structure of a Behavioral Access Program to provide perspective on why each of these layers is important to the health and wellbeing of first responders.
When looking at this framework and the implications that it may have for your organization, we encourage you to consider each layer of the pyramid as a level of care that can be provided to meet the behavioral health needs of your members. At the bottom of this pyramid is education. It may not be obvious at first as to why education is considered a level of care. However, we make the argument that education is the primary method by which we can care for our first responders because it is at this level that we have the greatest ability, and responsibility, to normalize mental health as human health, a state of existence universal to us all. Additionally, education is highly adaptable to the needs of your members depending on their roles, ranks, or other classifications. Furthermore, it increases general awareness of the effects of first responder service on mental health, as well as the avenues for support. Providing your members the foundational knowledge and skills relevant to them increases the likelihood that they will be able to successfully identify mental health concerns and then navigate your organization’s Behavioral Health Access Program to meet the need, whether that need be theirs, a family member or fellow first responder. Ultimately, education equals empowerment and empowered first responders are capable first responders.
The BHAP Framework
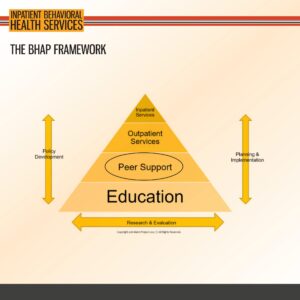
The next level of care that we will review is peer support. Just as with every other level of care within the Behavioral Health Access Program framework, there is a specific Toolkit module dedicated to the more in‑depth exploration of peer support. We encourage you to access that module if you are interested in learning more about the nature of peer support, why it is an imperative asset to any Behavioral Health Access Program, and ways in which to build or strengthen your organization’s peer support team.
However, for the purposes of this presentation, peer support is best explained as connection. More so, it is connection through shared life experiences. Often, members may find it difficult to share their mental health concerns with a family member, friend or even a medical or mental health professional, for fear that the person they are confiding in will not understand. With peer support, the difficulty that members experience is alleviated as they are sharing their concerns with another first responder, therefor they are sharing it with somebody who is likely to relate with what they’re going through. Peer support members serve as invaluable resources to their fellow first responders. In their work as a peer supporter, they provide members a safe, judgement free space in which to openly express their thoughts and feelings. They can take the raw and very real reactions that first responders have to various stressors and help them make sense of it through a lens of compassion and strength. They can help that member feel validated and restore their sense of self‑agency. Perhaps most importantly, they can reinforce the normalization of mental health in first responder service and, if needed, guide the member to higher levels of care.
The BHAP Framework
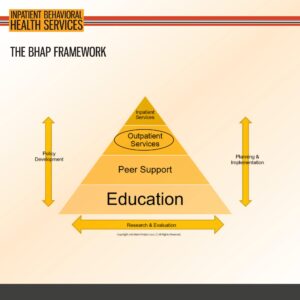
As mentioned previously, some of the content from the Outpatient Services module of the Toolkit is included within this presentation as both require a base understanding of the same core behavioral health concepts. More so, we will later include a side‑by‑side comparison of outpatient and inpatient services. As such, we will not belabor much on this level of care here. The key thing to remember about outpatient services in the broader context of the Behavioral Health Access Program, is that outpatient services are the first level of care at which members will seek professional behavioral health services. It is possible that, with a comprehensive and effective Behavioral Health Access Program in which members are provided strong support systems, foundational education, and early interventions, many members may never need to access professional mental health services. However, if they do, we must emphasize the importance of connecting your members with culturally competent providers who are appropriately qualified to work with first responders. First responders face unique stressors due to the nature of their professions. Not all mental health care providers are capable of meeting their needs with both empathy and evidence‑based interventions that will aid them in overcoming the mental health challenges they deal with. For more information about how to grow your outpatient services network, particularly when it comes to vetting potential providers, please refer to the Outpatient Services module.
The BHAP Framework
We have now reached the highest level of care, inpatient services, which will be the primary focus of this presentation. Though it is likely that few members will require support at this level, it is nonetheless an essential aspect to any comprehensive Behavioral Health Access Program. Inpatient services are typically reserved for members experiencing the most acute behavioral health concerns. These concerns can include, but are not necessarily limited to, intent to die by suicide or substance use severe enough to require medical detox. Though there is a strong argument to be made that the other levels of care, including education, peer support, and outpatient services, are immense protective factors that may help prevent a member’s mental health concerns from elevating to a degree requiring inpatient mental health services, these levels of care are not typically best for members actively dealing with concerns of this gravity. In what follows we will discuss other important aspects to inpatient services including how to determine when inpatient services are appropriate, special considerations to make when growing your inpatient network, and best practices for supporting a member who has recently discharged from inpatient services.
Behavioral Health: Why it Matters
Throughout the Toolkit, you will notice there is a strong message about how important behavioral health is in saving lives. As we learned in the preceding review, each level of the BHAP provides different knowledge, resources, interventions and prevention strategies to help improve mental health and reduce death by suicide. Given this, each level of care is necessary and important. It is at the inpatient level, however, that we can provide the most direct support to members who are experiencing the most critical need.
As first responders often transport individuals from the community to inpatient behavioral healthcare facilities, they are typically familiar with the providers and programs offered within their local area. Though this awareness may at first appear to be a benefit to members experiencing a critical mental health concern, it can serve as a significant barrier to care. Quite simply, members are reluctant to share their personal mental health concerns with the same providers with whom they have already established professional relationships. Though this is understandable, we know that inpatient facilities are a useful tool in the fight to save lives, especially in times of crisis. Thus, having these services vetted and ready for your members is imperative.
3. Inpatient Services Specifics
Audio
Transcript
Service Chart
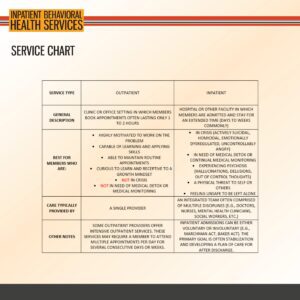
So, what is meant by inpatient services? Inpatient behavioral health services are those that are provided to an individual in a hospital or other designated inpatient facility, such as a receiving center. In these facilities, individuals in need of care are admitted, and typically spend at least one night, and sometimes longer, depending on the situation and assessment of the doctors or providers at the facility. Inpatient care can be both voluntary or involuntary. Patients at inpatient facilities are often under the care of an interdisciplinary team comprised of doctors, nurses, social workers, mental health clinicians, and other specialties depending on the presenting problems of the individual. Typically, a care plan and treatment goals for the inpatient stay are developed collaboratively with the patient. Often times the main goal is to stabilize the current crisis and develop a plan for continued care. This means that the goal of inpatient services is often to manage what is currently going on, which may not target the underlying cause of the issues. Most of the time inpatient services are used when symptoms are at high levels of intensity, frequency, and duration. Inpatient treatment can look very different at different programs. Programs may use individual therapy, group therapy, medical interventions, skills practice, art therapy, medication management, and other interventions deemed appropriate by the care team. Later we will discuss the questions to ask when vetting these inpatient care facilities. But for now, let’s look at the factors to consider when trying to determine if inpatient services are appropriate for your members.
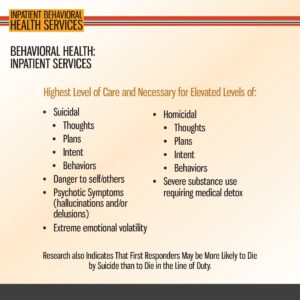
As we mentioned previously, inpatient services are the highest level of care and should be used when members are experiencing the highest level of need. In other words, inpatient services are typically indicated for members who are experiencing an active health crisis and thus, in some way, pose a threat to their own wellbeing or that of others. This could include the following situations: suicide‑related thoughts, plans, intent, or behaviors; homicide‑related thoughts, plans, intent, or behaviors; extreme emotional dysregulation or volatility, such as uncontrollable crying or rage; a member feeling unsafe to be left alone; active psychosis characterized by hallucinations and/or delusions; or the member having a severe substance use condition in which they would require medically monitored detox in order to safely obtain sobriety before treatment. How these concerns could potentially present is as varied and unique as the individuals themselves. However, that doesn’t mean it is impossible to identify and subsequently support a member in need of this level of care. Being aware of these signs is an important first step in getting your member the help they need and deserve. Another big step is being prepared. We highly encourage you to be proactive in learning about or helping to establish the protocols that will keep you and your members safe should they require inpatient services. Know where you can take them, who needs to be notified, and what information can be shared. Determine who is responsible for which actions and when those actions should take place. Knowing the processes and protocols in advance will mitigate the possibility of precious time being lost and distress being unnecessarily increased should a crisis occur and ultimately necessitate hospitalization. These judgement calls are never easy, but they are made less difficult by proper planning and conviction that inpatient services can save lives.
Behavioral Health: Inpatient Services
We want to make clear that suicidal thoughts are common and there are different levels of intensity and frequency that occur. Someone who has more morbid or passive suicidal ideation may have thoughts related to “If I went to bed and didn’t wake up in the morning, that’d be okay” or “I wish I were dead.” These thoughts are different than someone who has active suicidal ideation with a specific plan. Individuals who have this high frequency and intensity with action towards behaviors tend to need professional services and inpatient settings may be the best in an acute crisis. Those with more morbid or passive ideation may not need inpatient services at the time, although that will be an individual situation decision. Additional training for peer support on suicide specific interventions and assessment may help alleviate the concern with making this decision.
Growing Your Program
Now that we’ve discussed the nature of inpatient services and when this level of care is most appropriate, we will look at what you can do to start or grow your Behavioral Health Access Program as it relates to inpatient behavioral health care. This may feel like a difficult task, as choices of inpatient facilities are often limited within your community and, as we’ve discussed previously, first responders may be understandably reluctant to seek treatment at the same facilities where they already have professional ties established. However, our goal in this module is to provide you a framework to make the task of developing your inpatient program more manageable. Furthermore, we hope to provide you valuable guidance that will empower you to address these barriers successfully.
Shared here, the framework for implementing or improving the inpatient services component of your BHAP is broken down into 5 actionable steps. The steps include identifying the services and resources already available to your agency, familiarizing yourself with the services available and how to access them, developing a vetting process for inpatient service providers, developing a referral network that includes specialized programs for first responders, and establishing protocols to protect members experiencing behavioral health concerns. Though the real‑time implementation of this process may not be directly linear as the steps are listed here, referencing back to these steps as needed will provide you and your behavioral health team solid reference points that will be helpful when tackling this portion of growing your BHAP.
Identify the Resources Already Available to You
First responders are familiar with the concept of the scene size‑up. Upon responding to any call, one of the first things you do is determine what resources you have at your disposal to handle whatever the situation may be. The same is true when working to grow your Behavioral Health Access Program; it will save you valuable time and effort if you take time on the front end to identify what resources you and your department are already aware of and have access to. The most obvious of these possible resources from an inpatient services standpoint are likely those facilities in your area where you transport community members in crisis. We will later discuss ways to address the unique challenges associated with using these facilities for your members in need of inpatient services. But for now, knowledge is power and it is helpful to be familiar with these facilities as you never know when they may be the best option. Of course, it is helpful to consider other options, too. Here it is important to note that with increasing frequency, inpatient behavioral healthcare agencies are providing specialized programs that offer services unique to particular people or circumstances. This includes first responders. So, be sure to ask the agencies you work with already if they offer these types of programs or are familiar with any that do. It will strengthen your knowledge of what is already out there and available to you. And lastly, don’t forget to consider inpatient behavioral healthcare providers in surrounding communities. We will go into this more in depth later, but being aware of and well networked with these facilities is one great way to balance the personal versus professional dynamic of accessing inpatient care for first responders.

4. Special Considerations
Audio
Transcript
Special Considerations
Once you’ve identified the inpatient resources available to you and your department, it is important to familiarize yourself with each one. To be effective at helping a member in need of inpatient services, it is not necessary to be an expert on every single provider, program or facility out there. However, it can be incredibly helpful to have a general idea as to what services are offered by each resource, what limitations each resource has, and the procedures for accessing them. For instance, you would not want to send a member experiencing severe substance use concerns to a facility that does not offer medical care or is not otherwise equipped to provide for a safer detox, as the physiological withdrawal from certain substances can be deadly. So, upon identifying each potential resource, we challenge you to run each one through the following questions and track the answers per your BHAP protocols ‑ What do they do? What don’t they do? How can the resource be accessed? It is important that any follow‑up questions reflect the needs of your organization. Furthermore, it is also important to revisit this information periodically to ensure that it remains up to date and no changes need to be made in areas where this information is maintained or disseminated.
Similar to outpatient services, there are some standard qualities that you want to look for across inpatient service providers. You want to make sure that confidentiality is a top priority, that the inpatient facility and providers are committed to maintaining the privacy of the first responder, and that they inform the member of any limitations of confidentiality in an upfront, direct manner. This can help build trust in the program and alleviate anxiety the member may feel about their mental health concerns or other personal information being shared with others who do not need to know. You also want to assess for cultural competency of the program and its providers. Does the program have providers who are knowledgeable about the customs, beliefs, and values of first responders? Though it is not necessarily a hard requirement that providers be directly familiar with first responder service or the unique challenges they face as a result of their professions, knowledge of these factors can help reduce barriers to treatment and improve outcomes for your members. And lastly, you want programs and facilities that are easily accessible. In other words, services at inpatient facilities should be affordable and easy to reach. Additionally, admissions processes should be designed to reduce possibilities of unnecessary stress exacerbating the member’s crisis. Though it will be up to you and the rest of your Behavioral Health Access Program team to determine other qualities that providers, programs and facilities must possess in order to be considered a part of your network, we argue that these 3 qualities are non‑negotiable and should be prioritized at all times.
Vetting Inpatient Providers or Facilities: What to Ask
When vetting a potential inpatient services provider, program or facility there are several questions to ask to determine if they are likely to be a good fit for the needs of your members and organization. Furthermore, it is important to understand the implications and possible consequences associated with the responses you receive. For example, awareness of the insurances accepted, if any, can help reduce the chance of a first responder feeling like they must choose between their mental wellbeing and the financial security of their family. As another example, knowing the treatments offered and the professional discipline of the providers can aid immensely in communication with the member and in coordinating follow‑up care after discharge.
Ultimately, the specific questions asked in your vetting process should be determined by you and the rest of your BHAP team, as you are the ones most familiar with the unique needs of your members. The questions listed here and on the next slide, much like the qualities listed previously, are recommended as the bare minimum. Asking additional questions through the lens of what is meaningful to your organization and its members is essential.

Vetting Inpatient Providers or Facilities: What to Ask
Listed here are additional questions to consider when vetting potential inpatient providers, programs or facilities. In addition to questions specific to treatment and processes, you will notice that this group of questions also encourages you and your BHAP team to consider what you can do to facilitate a mutually beneficial relationship founded on respect and reciprocity of care. This is a crucial aspect to building and maintaining the professional relationships between organizations and individuals that ensures first responders receive the highest quality care in the most expeditious and effective manner possible. Beyond that, it serves as an opportunity to expand your network, increase your access to additional resources, and normalize all levels of mental health care.
Asking these questions is just part of the vetting process. After receiving the responses, it will be up to you and your organization’s Behavioral Health Access Program team to determine who passes the standards you’ve set forth. Though having multiple options is rarely a bad thing, there is something significant to be said about quality over quantity, particularly when it comes to inpatient mental healthcare providers. After asking these questions, and any additional ones your team has settled on, then you will be ready to formally establish your referral networks as you will have put in the work to identify who you’d send your members to, as well as who you would not. Members aware of the work that went into vetting the providers to whom they are being referred are far more likely to approach inpatient services with an open mind and access various levels of care again should they require it in the future.

5. Barriers and Continuity of Care
Audio
Transcript
Barriers
Though we’ve already mentioned several barriers to members accessing inpatient behavioral health care services, we feel that those shared here bear repeating. We know that these barriers have the ability to strongly influence outcomes toward the negative. To reduce the power of these barriers we encourage you and your department to take a proactive stance in developing the protocols that will help protect the member in need of support, members serving in supportive roles and the organization as a whole. Do not wait until you are directly faced with a high stakes situation in which a member is in crisis to determine what is expected or what resources are available. Instead, do your homework now! Reach out to other organizations and find out what they have done to support their members in times of critical need. Ask for examples of standard operating procedures and guidelines and then be willing to have the necessary conversations among your BHAP team members and leadership to determine how they can be adapted to meet the needs of members and the organization best. Develop protocols that provide protections for those members who are brave enough to seek help. Providing them assurance in writing that they will be supported and their jobs will be protected increases the likelihood they will consider help if they need it. Partner with facilities in neighboring counties or cities so that your members can receive inpatient treatment at locations other than those they transport to. Discuss confidentiality procedures with these facilities and if there is a possibility of providing care to an “anonymous” first responder. Run your BHAP team and other supporting members through realistic training scenarios where they must respond to a member in critical need. Furthermore, brainstorm more ideas about how to overcome the barriers to care that you and your Behavioral Health Access team have discovered.
Considering what to do in the event a member needs inpatient behavioral health services is imperative. However, equally important is determining what the organization and supporting members can do after the member in need of support has discharged from the inpatient stay. Post-discharge is a highly vulnerable time for many individuals. As mentioned previously, the goal of inpatient services is often just to stabilize the immediate crisis. Inpatient stays or hospitalizations, even extended ones, may be too brief in nature to fully address all the underlying concerns that contributed to the crisis occurring. Upon discharge, members may be facing scary, confusing, unfamiliar, or simply stressful circumstances such as trying to coordinate outpatient mental health treatment, adjusting to new medications, or dealing with unresolved stressors that have only intensified in their absence. Thus, we must again be proactive in identifying the ways and means by which we will continue to provide support to members once they leave inpatient services and attempt to integrate back into their “normal” life and work routines.
Post-Discharge is Important
Post‑discharge support is likely to be the most effective if it is comprehensive in nature. Or in other words, it can be helpful for support to come from multiple sources within the organization. One potential resource is peer support. Peer support is already an incredibly valuable tool that leverages the strengths of shared experience to foster connection. Even if the peer support member cannot relate to participating in inpatient services before, they can likely relate to the reasons contributing to the other member doing so. As such they can serve a crucial role in mentoring that member and making that them feel validated and heard. Peer support members can also aid the member in coordinating post discharge care and requirements to return to work. They can serve as a liaison between the member and the department until the member is capable of navigating this relationship on their own again. And this leads us to the next element of post-discharge that is incredibly important – a return to work plan! Here is another aspect where being proactive is essential to the effective support of your members. BHAP teams should work to develop and formally establish policies to aid members in their transitions back to work. This may include considering ways to gradually stair step the member back into their typical role. It may also include processes for getting the member connected to an already vetted and culturally competent outpatient mental health care provider. Lastly, don’t forget to keep perspective. Imagine yourself in the place of the member facing the challenges of post-discharge. Think about how stressful it may be and all the changes they may face in addition to everything else. What would it feel like to be in their shoes? Approach the member with empathy and remember that experiencing a temporary mental health crisis is not a reflection of weakness or incompetence. Keep the member involved and informed. They deserve it and they will provide you valuable insight.
Continuity of Care is Critical
On a closing note, we emphasize that continuity of care is critical. In this we must also clarify that the term “care” is used here in a broad way that encompasses not only mental health services provided by mental health professionals on an inpatient or outpatient basis, but equally so, by you and the organization. Members who feel supported by their fellow team members, leadership, community members, families and others are more likely to experience positive mental health outcomes. Thus, we encourage BHAP teams to consider how they can increase their outreach and reinforce support networks at all possible levels. In addition to the formal aspects of care, like a care plan that outlines the next steps for treatment or a return to work plan that aids transition following inpatient discharge, it is also imperative that we informally follow-up with members, too. Follow up should be thorough, frequent, and sincere. Approach from a place of empathy and compassion. Though members may benefit from a space in which they can openly discuss their mental health concerns, they don’t need to be coddled or reminded constantly that they areas of their wellbeing they need to work on. Overall, the organization has an opportunity to provide needed support and normalize mental wellbeing and mental health care at all levels for all members. Doing so will save lives.
Resources
Thank you for reviewing this module. Please see the below resources for additional information on the included topics.